
Myeloma Morning: Survival & Age, Once-Weekly Kyprolis, And Revlimid & Neutropenia

Hello, myeloma world.
We hope your week has gotten off to a great start.
We're looking forward to reviewing three new myeloma-related research studies with you today.
The first study we summarize in today's report focuses on the survival of older blood cancer patients, including (of course) older multiple myeloma patients.
The second study presents the results of the CHAMPION-1 clinical trial, which tested once weekly Kyprolis in combination with dexamethasone in relapsed multiple myeloma patients.
The final study we review is a detailed look at an important Revlimid-related side effect – neutropenia, or low levels of neutrophil white blood cells. The study summarizes results of an observational trial that was carried out to track the occurrence of severe neutropenia in relapsed myeloma patients treated with Revlimid.
Before we start with today's research summaries, we want to take a moment to thank the Beacon's newest sponsor, the Seattle Cancer Care Alliance (SCCA). Sponsors such as SCCA makes it possible for The Beacon to continue providing reliable, up-to-date news and support to the multiple myeloma community worldwide.
We are particularly grateful to SCCA for the generosity of its support. SCCA is the first myeloma treatment center to support the Beacon's work at one of our higher sponsorship tiers.
Survival Of Older Multiple Myeloma Patients
A team of researchers based in Germany has investigated recent trends in the survival of older blood cancer patients in the United States – including older multiple myeloma patients (abstract).
The researchers find that the survival of U.S. multiple myeloma patients of all ages has increased significantly in the last 20 years. However, the survival of older myeloma patients is still much less than the survival of younger myeloma patients.
The researchers used data from the U.S. National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) database, the most important compendium of U.S. cancer statistics, for their calculations.
Specifically, the researchers used the SEER data to calculate five-year relative survival rates for patients who were 65 years old or older and were diagnosed with a common hematologic malignancy (such as various forms of leukemia or lymphoma, and multiple myeloma) between 1992 and 2012. They calculated the survival rates for the following four periods: 1997-2000, 2001-2004, 2005-2008, and 2009-2012. For the sake of comparison, the researchers included five-year relative survival rates for patients aged 50 to 59 years.
Again, just to be clear, the focus of this study was relative survival rates, rather than the absolute survival rates one typically reads about in most studies reporting, for example, clinical trial results. Relative survival is a measure of survival adjusted for the survival that would have been expected for a group of patients given their age, gender, race, and other characteristics. Absolute survival, in contrast, is not an adjusted metric – it is simply the percent of patients who survive for a certain period of time after they have been diagnosed (or after some other milestone).
For a more detailed description of the difference between relative survival and absolute survival, please see the background information at the end of this previous edition of Myeloma Morning.
Overall, data from 355,972 patients, including more than 62,000 patients with multiple myeloma, were the basis for the analysis in the new study. The authors use a modeling-based approach for estimating relative survival in each period of their study. This allowed them to estimate relative survival rates for periods of time – such as the 2009-2012 period – when actual five-year survival rates are not yet available.
Based on their analysis for all the patients in their dataset, and across types of blood cancer, the authors conclude that
“Newer therapies and a better understanding of how to treat older patients have led to increased survival expectations for older patients with most hematologic malignancies, but an age-related survival disparity persists.”
In the case of multiple myeloma, the researchers observed a significant increase in five-year relative survival for patients of all ages (see the graph below). The improvement was particularly marked for patients 65 to 69 years of age at diagnosis, and also for 75 to 79 year-olds.
Unfortunately, the smallest survival improvement occurred in the group with the lowest relative survival – patients who were 85 and older at diagnosis. In the last period of the study, the five-year survival of this group of patients was less than one fifth the survival of people of the same age, but who do not have multiple myeloma
(click on image for full-size version)
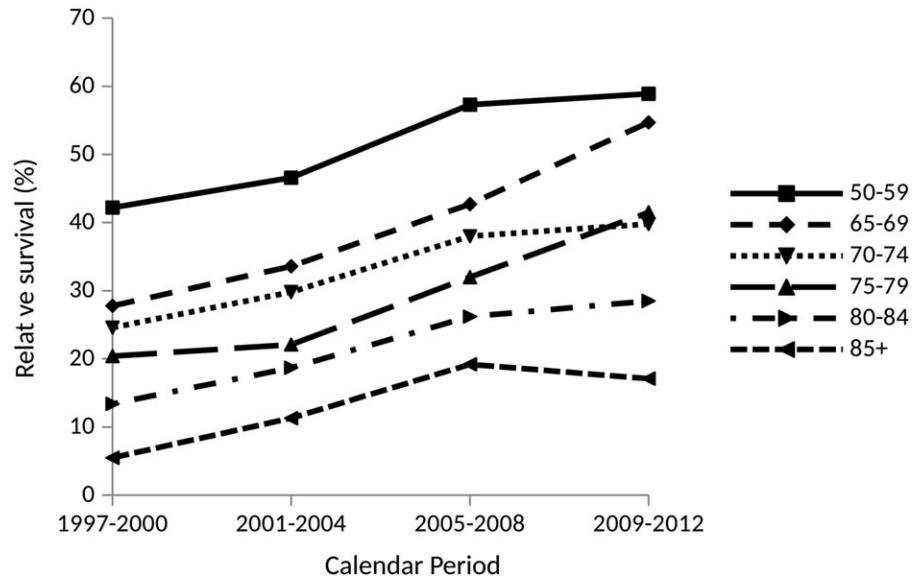
Source: Pulte, D. et al., “Changes in the survival of older patients with hematologic malignancies in the early 21st century” in Cancer, May 10, 2016.
Once Weekly Kyprolis – Results Of The CHAMPION-1 Clinical Trial
Results of the CHAMPION-1 trial were published last week in the journal Blood (abstract). The trial evaluated the safety and efficacy of once weekly, higher-dose Kyprolis (carfilzomib) with dexamethasone in patients with relapsed and refractory multiple myeloma.
The researchers carried out the trial because being able to administer Kyprolis just once per week, instead of the standard two times per week, could make Kyprolis a more convenient treatment option for many patients.
Overall, 116 patients were recruited across 32 sites in the Unites States for the single-arm CHAMPION-1 study. The results summarized in the new research article about the trial are based on data from the 104 patients who were treated at the maximum tolerated dose (70 mg/m2) established during the Phase 1 portion of the trial.
The Kyprolis dosing in the trial was 20 mg/m2 for the first infusion, then 70 mg/m2 per infusion thereafter. Kyprolis was administered as a 30-minute intravenous infusion once a week for three out of four weeks.
In comparison, the most common approved Kyprolis dosing in the U.S. and in Europe is 20 mg/m2 per infusion initially, followed by just 27 mg/m2 (if the 20 mg/m2 dose is tolerated). This dosing is for Kyprolis administration twice per week for three weeks out of a four-week cycle. With this dosing, the infusion time per infusion can be as little as 10 minutes.
There also is an approved dosing in the United States for Kyprolis either as a single agent, or in combination with dexamethasone, where the initial dose of Kyprolis is 20 mg/m2 per infusion, followed by 56 mg/m2 (again, if the initial 20 mg/m2 dose is tolerated). As with the lower Kyprolis dose, this approved dosing is for administration twice per week for three weeks out of a four-week cycle. At this dosing, the infusion time per infusion should be at least 30 minutes.
The median age of the 104 patients in the CHAMPION-1 trial was 69 years. The study participants had received a median of one previous therapy, but could have up to three prior therapies; 83 percent of the patients were previously treated with Velcade, and half were previously treated with Revlimid.
More than three quarters of the patients (77 percent) responded to treatment, with 3 percent achieving a stringent complete response, 11 percent a complete response, 33 percent a very good partial response, and 31 percent a partial response.
Median treatment duration was 7.7 months.
The median progression-free survival was 12.6 months.
The most common severe side effects included fatigue (11 percent), hypertension (7 percent), pneumonia (6 percent), acute kidney damage (6 percent), low platelet counts (6 percent), and anemia (6 percent). Hardly any patients experienced peripheral neuropathy as a result of treatment.
Two patients died during the study due to Kyprolis-related adverse events – one was due to a case of acute respiratory distress syndrome, and the other was due to cardiopulmonary arrest. In both cases, the patients had a history of high blood pressure and developed pneumonia during the study.
Almost three quarters of patients (72 percent) discontinued treatment; 35 percent discontinued due to disease progression, 24 percent due to patient or physician choice, and 12 percent due to adverse events.
The researchers conclude that, based on results of the trial, once-weekly, higher-dose Kyprolis in combination with dexamethasone “appears to be feasible, generally well tolerated, and active for patients with relapsed or relapsed and refractory multiple myeloma.”
Based on the results of the trial, the Phase 3 trial “ARROW” has been initiated to compare the efficacy and safety of once weekly 20 / 70 mg/m2 Kyprolis plus dexamethasone to twice weekly 20 / 27 mg/m2 Kyprolis plus dexamethasone in relapsed myeloma patients.
Revlimid And Severe Neutropenia In Relapsed Multiple Myeloma
An international team of myeloma researchers has published results of an observational study of Revlimid (lenalidomide) in the treatment of relapsed multiple myeloma patients. The study focused on the occurrence of a particular side effect – neutropenia, or low levels of neutrophil white blood cells (abstract).
Neutropenia is a well-known side effect of Revlimid treatment. In severe cases of the side effect, doctors often must reduce the dose of Revlimid the patient is receiving, or suspend treatment with the drug until the side effect subsides.
Due to the impact neutropenia can have on treatment with Revlimid, a team of researchers decided to investigate how often severe (grade 3 or grade 4) neutropenia occurs in patients treated with Revlimid, and how the side effect is managed.
The researchers organized an observational study, known as the “IMPACT MM,” which was conducted in 34 different treatment centers in nine countries, mainly in Europe. Patients were recruited for the study if they had relapsed, or relapsed and refractory, multiple myeloma. They were treated with Revlimid and dexamethasone; combination therapy with an additional anti-myeloma agent was not permitted while patients were taking part in the study.
Study participants were tracked for up to 12 months after the start of treatment, or until they halted the Revlimid and dexamethasone treatment.
A total of 198 patients eventually took part in the study. They had a median age of 70, were a median of 3 years from the time of their diagnosis, and had a median of two prior lines of therapy. A bit more than a third of the patients had undergone a stem cell transplant.
Patients were treated with Revlimid and dexamethasone a median of 9.1 months during the study.
During their time on treatment, 31 percent of the patients experienced at least one case of severe (grade 3 or 4) neutropenia.
Among the patients who experienced severe neutropenia, the median time until it occurred was 8.8 weeks after the start of treatment with Revlimid and dexamethasone.
If a patient experienced severe neutropenia early during their treatment, they were very likely to experience it again. Among the patients who experienced severe neutropenia during their first or second cycle of treatment, 81 percent experienced it again.
More broadly, about half the patients who experienced one case of severe neutropenia experienced it at least one additional time.
Despite the fact that almost a third of the patients in the study developed severe neutropenia, only a small number of patients (about 3 percent) developed febrile neutropenia, an especially serious form of neutropenia where the low neutrophil level is accompanied by a fever.
Similarly, the cases of neutropenia observed during the study accounted for only a small number of the unplanned hospitalizations patients experienced during the study.
Severe neutropenia was more likely to occur in patients who had relapsed and refractory myeloma, rather than just relapsed myeloma. The side effect also was seen more often in patients with reduced kidney function.
About three quarters of the patients who developed severe neutropenia were treated at least once with a granulocyte colons stimulating factor (GCSF) such as Neupogen (filgrastim). In most cases, treatment with GCSF was for just a single day.
New Myeloma-Related Research Articles
- Berenson, J. A. et al., “CHAMPION-1: a phase 1/2 study of weekly carfilzomib and dexamethasone for relapsed or relapsed and refractory multiple myeloma” in Blood, May 12, 2016 (abstract)
- Deighan, W. I. et al., “Annals Express: Multiple myeloma and multiple plasmacytomas associated with free gamma heavy chain, free kappa light chain and IgGk paraproteins: An unusual triple gammopathy” in Annals of Clinical Biochemistry, May 10, 2016 (abstract)
- Dutoit, J. C. and Verstraete. K. L., “MRI in multiple myeloma: a pictorial review of diagnostic and post-treatment findings” in Insights into Imaging, May 10, 2016 (full text)
- Leleu, X. et al., “An international, multicenter, prospective, observational study of neutropenia in patients being treated with lenalidomide + dexamethasone for relapsed or relapsed/refractory multiple myeloma (RR-MM)” in American Journal of Hematology, May 11, 2016 (abstract)
- Mikulasova, A. et al., “Genome-wide profiling of copy-number alteration in monoclonal gammopathy of undetermined significance” in the European Journal of Haematology, May 9, 2016 (abstract)
- Pulte, D. et al., “Changes in the survival of older patients with hematologic malignancies in the early 21st century” in Cancer, May 10, 2016 (full text)
- Reece, D. E. et al., “Cyclophosphamide and bortezomib with prednisone or dexamethasone for the treatment of relapsed and refractory multiple myeloma” in Clinical Lymphoma, Myeloma & Leukemia, May 9, 2016 (abstract)
- Tetsuro, Y. et al., “Receptor-activator of nuclear kappaB ligand expression as a new therapeutic target in primary bone tumors” in Plos One, May 10, 2016 (full text)
- Van De Donk, N. W. C. J. et al., “Diagnosis, risk stratification and management of monoclonal gammopathy of undetermined significance and smoldering multiple myeloma” in the International Journal of Laboratory Hematology, May 9, 2016 (full text)
Related Articles:
- None Found
