
Early Or Late Stem Cell Transplantation For Myeloma? New Study Finds Both Strategies Yield Similar Overall Survival

Results from a retrospective study show that delaying stem cell transplantation following initial therapy may result in shorter progression-free survival following transplantation compared to transplantation soon after diagnosis.
However, the results also show that the timing of transplantation does not significantly impact overall survival.
The median progression-free survival after transplantation was 28 months for those who underwent early transplantation (within 12 months of diagnosis) compared to 18 months for those who underwent delayed transplantation (more than 12 months after diagnosis). This difference was not statistically significant, but the study investigators explain that this is probably due to the fact that the number of patients included in the analysis was small.
Despite progression-free survival appearing better when transplantation is done early, transplant timing did not significantly affect overall survival.
These findings are consistent with several other studies that have investigated the optimal timing of stem cell transplantation in the era of novel anti-myeloma agents. One study, however, found that early stem cell transplantation prolonged overall survival.
Given that there is still no clear answer whether stem cell transplantation is best done soon after diagnosis or whether it can be delayed without impacting outcomes, several ongoing prospective randomized clinical trials are examining the optimal timing for stem cell transplantation.
Background
High-dose therapy followed by autologous stem cell transplantation was introduced as a potential treatment for multiple myeloma in the 1980s. By the late 1990s and early 2000s, it had become a standard treatment for younger and healthier myeloma patients.
Over the past 15 years, however, studies have shown that novel anti-myeloma agents – such as thalidomide (Thalomid), Revlimid (lenalidomide), and Velcade (bortezomib) – extend the progression-free and overall survival of myeloma patients. Due to the efficacy and high tolerability of the novel agents, many myeloma patients in recent years have been choosing to delay or forego stem cell transplantation.
Therefore, there has been a large interest in, and need for, studies that investigate the optimal timing of stem cell transplantation in the era of novel agents.
To address this need, researchers have recently starting comparing survival outcomes of myeloma patients who underwent early versus late transplantation.
Study Design
Researchers from the Ohio State University retrospectively analyzed results from 167 myeloma patients who underwent high-dose chemotherapy and autologous stem cell transplantation at their center between 2002 and 2009 and who had received initial therapy with thalidomide, Revlimid, or Velcade.
Among these patients, 61 percent underwent early transplantation within 12 months of their myeloma diagnosis, and 39 percent underwent delayed transplantation more than 12 months after their diagnosis.
No patients received consolidation or maintenance therapy after transplantation.
The median patient ages were 57 years for those who underwent early transplantation and 55 years for those who underwent late transplantation.
Among those who underwent early transplantation, the median time to transplantation was 7.9 months after diagnosis. For those who delayed transplantation, the median time to transplantation was 17.7 months after diagnosis.
Both groups of patients had similar exposure to induction therapy with Revlimid (33 percent of the early transplant group and 28 percent of the late transplant group), but the early transplant group had more patients who had received Velcade-based therapy (63 percent versus 49 percent) and the late transplant group had more patients who had received thalidomide-based therapy (66 percent versus 38 percent).
There was no significant difference in the share of patients in each group who had standard versus high-risk cytogenetics (chromosomal abnormalities). In both groups, about two thirds of the patients had standard-risk cytogenetics.
The median follow-up time was 31 months from diagnosis and 23 months from transplantation for the early transplant group, and 52 months from diagnosis and 29 months from transplantation for the late transplant group.
Study Results
Nearly all patients achieved at least a partial response as a result of their transplantation, regardless of the timing (99 percent of patients who underwent early transplantation and 97 percent of patients who underwent late transplantation).
However, patients who underwent early stem cell transplantation achieved deeper responses. Half of the patients who underwent early transplantation achieved a complete response and 27 percent achieved a very good partial response. In comparison, 28 percent of those who delayed transplantation achieved a complete response and 28 percent achieved a very good partial response.
At the time of the study analysis, 40 percent in the early transplant group had relapsed, compared to 55 percent in the late transplant group. The median time to relapse was 28 months for the early transplant group and 23 months for the late transplant group.
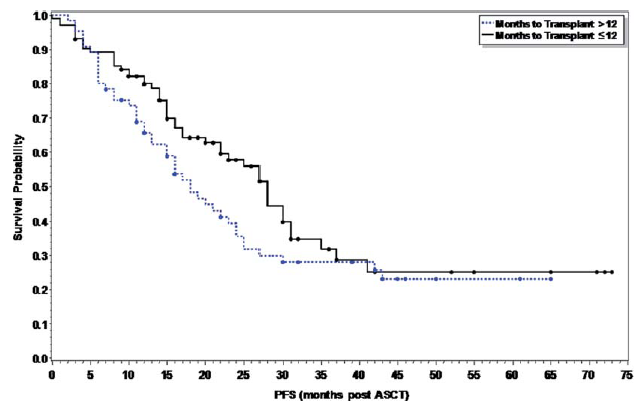
Progression-Free Survival (Solid Line = Early-Transplant Patients)
Click on image to view a larger version of it.
Overall, the median progression-free survival was longer in the early transplant group (28 months versus 18 months), but the difference was not considered statistically significant.
(Click here or on the image to the right to see a larger graph of the key progression-free survival results.)
Among high-risk patients, though, median progression-free survival was significantly longer when transplantation was performed early in the course of the disease (25 months versus 11 months).
The treatment-related death rate 100 days post-transplant was 3 percent for the early transplant group and 0 percent for the late transplant group. At one year post-transplant, the treatment-related death rate was 4 percent for the early transplant group and 1.5 percent in the late transplant group. All treatment-related deaths were due to infection.
Three years after diagnosis, the overall survival rate was 90 percent for those who underwent early transplantation compared to 82 percent for those who delayed transplantation. However, five years after diagnosis, the overall survival rate was 63 percent for both groups.
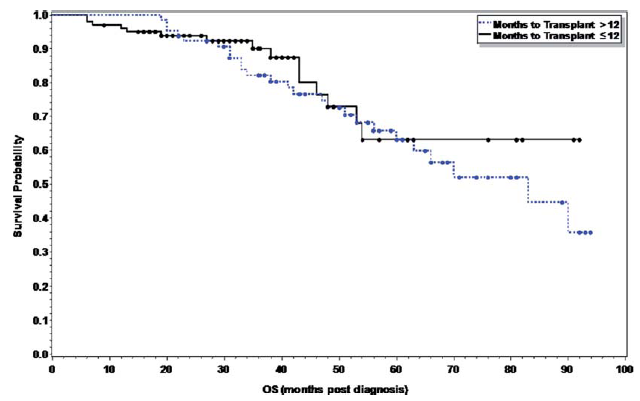
Overall Survival (Solid Line = Early-Transplant Patients)
Click on image to view a larger version of it.
Additionally, the median overall survival was not yet reached in the early transplant group and was 83 months for the late transplant group; this difference, however, was also not considered statistically significant.
(Click here or on the image to the right to see a larger graph of the key overall survival results.)
Predictive factors for disease progression after transplantation included stage III disease – according to the International Staging System (ISS) – and not achieving at least a very good partial response after transplantation. Patients on hemodialysis, a treatment for kidney disease, had poorer overall survival. Choice of novel agent did not affect progression-free or overall survival.
For more information, please refer to the study in the journal Leukemia & Lymphoma (abstract).
Related Articles:
- None Found
This is a really interesting article and I'm surprised more people haven't commented on it.
Although it is true that statistically the two treatment approaches were not very different from each other when it comes to the key result (overall survival), it sure seems to me that the overall survival graph suggests early transplant may be more beneficial in the long term compared to a late transplant.
I say that, by the way, as someone who has not yet had a transplant. I'm not here to go rah rah about the strategy I took.
But look at the flat section after five years or so for the early transplant patients in the overall survival graph, when the survival curve for the late transplant patients keeps going down.
My daughter was diagnosed with stage III multiple myeloma in April 2013. She had three events of neutropenia (?) which interrupted treatment each event. The novel drug initially was Velcade, which caused a fever incident, and recently Revlimid at half the normal dose, which reduced her immunity to almost 0, so was discontinued after one week. This week she has been on no chemotherapy at all. This week she returns for more lab work, but I am concerned about what treatment will now be. She was never at a level appropriate for stem cell although was told because of her general fine health and age 49, she would be a candidate. So, too late? That is a dour thought. I should be the one with cancer -- 87 years old -- not she. She will be in the late stem cell group it appears, this does not look like a positive outcome.
I think more study should be done on hormones relative to multiple myeloma. I have read a bit on this but my instinct tells me it was relevant in my child's case but no one seems interested in this possibility.
fbs
Thanks for your comment, Faith. We're sorry to hear about the problems your daughter has been having with treatment for her multiple myeloma.
Although we understand your concern, you should know that there are many options your daughter can pursue for the treatment of her myeloma. It is also possible that her doctors will figure out ways to treat her with Velcade or Revlimid despite the problems she has had with the treatments so far.
Is your daughter's treatment being guided by a physician who specializes in multiple myeloma. Most specialists are at major cancer centers. Given the challenges she has had so far with her treatment, it would be particularly advisable for her to be seen by a myeloma specialist.
Good luck, and please update us on how your daughter is doing -- here, or in the Beacon's discussion forum,
http://www.myelomabeacon.com/forum/
Get new Myeloma Beacon articles by email.