Minimal Residual Disease, Deep Sequencing, And Prognosis In Multiple Myeloma
By: Navneet Ramesh; Published: April 8, 2014 @ 7:41 am | Comments Disabled
A recent Spanish study adds important findings to the growing literature about the measurement and significance of minimal residual disease in multiple myeloma.
Myeloma patients are said to have minimal residual disease if, after having responded well to treatment, they nevertheless continue to have myeloma cells in their bodies.
In their study, the Spanish researchers used a sensitive new technique known as deep sequencing to conduct minimal residual disease testing. They used the technique to test for residual disease in bone marrow samples from myeloma patients who had completed their first line of therapy and achieved at least a very good partial response.
Patients who had no signs of residual disease based on deep sequencing had markedly longer progression-free and overall survival than other patients.
In addition, among patients who had residual disease after initial treatment, the extent of the residual disease had a noticeable impact on survival. Patients with lower levels of residual disease had longer progression-free and overall survival than those with higher levels of residual disease.
The investigators also demonstrated that testing using deep sequencing provides results that, in a large majority of cases, are the same as those of more common, but less sensitive, testing methods such as multiparameter flow cytometry.
However, in cases where the results from deep sequencing and multiparameter flow cytometry differed, the deep sequencing results provided a better guide to patient prognosis.
Although their results underscore the potential value of deep sequencing for minimal residual disease testing, the Spanish investigators recognize that the technique has its limitations. Myeloma cells, for example, are not uniformly distributed in the bone marrow. Thus, even when sensitive tests fail to detect residual disease in a bone marrow sample, there may still be myeloma cells elsewhere in the patient's body.
The researchers therefore suggest that additional methods, such as imaging techniques and monitoring of circulating myeloma cells, be used to assess disease status and improve estimates of the risk of progression.
They add that the detection of minimal residual disease by deep sequencing may also contribute to the design of patient-specific treatment approaches, such as discontinuation of treatment for patients without residual disease, or intensification of treatment for patients with minimal residual disease
Background
Due to the progress that has been made in the treatment of multiple myeloma in the last decades, the share of newly diagnosed patients who achieve a complete response following treatment has increased significantly.
However, almost all myeloma patients eventually relapse after initial treatment. Most of these relapses, the Spanish researchers say, "can be attributed to the persistence of undetectable minimal residual disease."
The term "minimal residual disease [1]" (MRD) is used to describe the presence of small numbers of myeloma cells in a patient's body even after the patient has achieved a complete (or very good partial) response to a treatment.
Traditionally, MRD testing in multiple myeloma patients has been carried out using cells from bone marrow samples. It is also possible, however, to conduct such testing using cells from the blood.
Patients who have no detectable myeloma cells in their cell samples are described as being MRD-negative. Patients with at least some myeloma cells in their samples are categorized as MRD-positive.
One established method for measuring MRD in myeloma patients is a technique called multiparameter flow cytometry.
However, according to the Spanish researchers, there is still room for improvement in the detection of minimal residual disease.
They therefore evaluated the prognostic value of a newer, more sensitive, method of minimal residual disease detection called deep sequencing. While multiparameter flow cytometry currently has a sensitivity of between 1 out of 10,000 and 1 out of 100,000 cells tested, deep sequencing is sensitive to levels up to 1 out of 1,000,000 cells tested.
(In the literature about MRD testing, a sensitivity of 1 out of 10,000 is often described using the shorthand 10‑4. A sensitivity of 1 out of 1,000,000, for example, would be labeled 10-6.)
The deep sequencing approach to MRD testing gets its name from the fact that it involves sequencing, which is the process of determining the genetic makeup of a cell. Deep sequencing is when the sequencing process is carried out multiple times for each single cell tested, which increases the accuracy of the testing.
When deep sequencing is used for MRD testing for myeloma, pre-treatment samples are first analyzed to identify a genetic sequence characteristic of an individual patient's disease. This sequence is then looked for in post-treatment samples from the patient to differentiate between myeloma cells and normal cells.
Study Design
In the current study, the Spanish investigators deep sequenced bone marrow samples from 133 multiple myeloma patients who had participated in several different clinical trials in Spain.
The samples used for most of the analyses during the study were obtained after the patients had completed their first line of therapy. For patients under the age of 65, the first line of therapy included induction therapy followed by a stem cell transplant. For patients 65 and older, the first line of therapy included only induction therapy without a stem cell transplant.
Only patients who achieved at least a very good partial response following their first line of therapy were included. The mean patient age was 62 years old.
All patients also had their MRD levels measured through multiparameter flow cytometry.
Initial findings from the current study were presented at the ASCO 2013 meeting (see related Beacon [2]news).
Study Results
The investigators first deep sequenced bone marrow cells that were taken from the patients prior to their starting treatment for their myeloma. They were able to identify myeloma cell-specific genetic sequences in 91 percent of patients, making them eligible for later MRD testing using deep sequencing.
During follow-up, the majority of patients (73 percent) remained MRD-positive, where MRD-positive was defined as having more than 1 myeloma cell out of 100,000 cells tested.
MRD Status And Patient Prognosis
Patients who were MRD-negative after their first line of therapy had a significantly longer median time to disease progression (80 months) than patients who were MRD-positive (31 months).
Median overall survival was also significantly longer in MRD-negative patients (not yet reached), compared to MRD-positive patients (81 months).
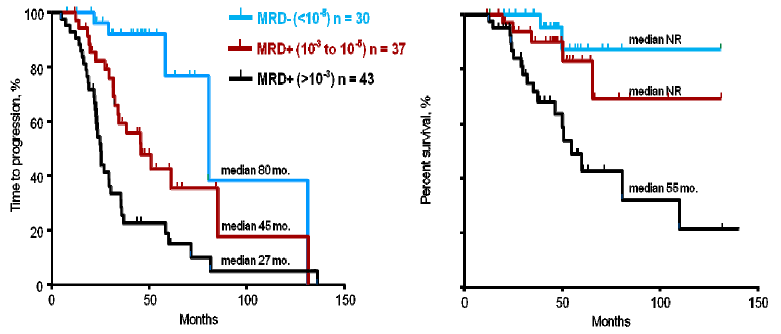
Patients were subsequently divided into three groups according to their MRD levels identified by deep sequencing: MRD levels of greater than 1 myeloma cell out of 1,000 cells; MRD levels between 1 out of 1,000 and 1 out of 100,000; and MRD levels of less than 1 out of 100,000 (MRD-negative).
The investigators found that the median time to progression varied significantly among the three groups (see graph on the left in the figure below). Patients who were MRD-negative (less than 1 out of 100,000 cells tested) had the longest median time to progression (80 months), followed by patients with MRD levels between 1 out of 1,000 and 1 out of 100,000 cells (48 months), and patients with MRD levels greater than 1 out of 1,000.
The investigators made similar observations for overall survival (see graph on the right in the figure below). Median overall survival was not yet reached for MRD-negative patients (less than 1 out of 100,000) and for patients with MRD levels between 1 out of 1,000 and 1 out of 100,000, compared to 55 months for patients with MRD levels greater than 1 out of 1,000 (27 months).
 [3]
[3]Time to Progression (left) and Overall Survival (right)
(click on image to view a larger version of it)
When the investigators limited the analysis to patients who had achieved a complete response to first-line therapy, they found that patients who were MRD-negative had a significantly longer median time to progression compared to MRD-positive patients (131 months versus 35 months). The median overall survival was not reached in either group.
Comparisons With Other MRD Testing Techniques
The researchers also compared MRD information obtained by deep sequencing with the results from multiparameter flow cytometry testing. They found that 83 percent of the samples yielded results that were the same using the two methods: 61 percent of samples were MRD-positive, and 22 percent were MRD-negative.
They also found an overlap in 85 percent of the patients when comparing MRD results based on deep sequencing with MRD results obtained using a third type of MRD testing, known as allele specific oligonucleotide - polymerase chain reaction (ASO-PCR).
For patients whose samples resulted in different MRD results using deep sequencing and multiparameter flow cytometry, the patients who were MRD-negative by deep sequencing had a longer time to disease progression than those who were MRD-negative by multiparameter flow cytometry but MRD-positive by deep sequencing (median not reached versus 50 months).
According to the Spanish investigators, their results suggest that low-level MRD results detected by deep sequencing are clinically significant.
For more information, please refer to the study by Martinez-Lopez, J. et al., “Prognostic value of deep sequencing method for minimal residual disease detection in multiple myeloma,” in Blood, March 11, 2014 (accepted) (abstract [4]).
Update (Apr 8, 2014 - 4:35 pm) - This article has been revised slightly from its original version. The primary change was to the description of how deep sequencing detects myeloma cells during MRD testing. The original version of the article suggested that the testing is done by looking in cells for myeloma-related genetic patterns that are common in myeloma patients in general. That is not correct. Instead, the patterns that are used for the detection of myeloma cells are patient-specific. For each patient, the myeloma-related genetic patterns are established by analysis of a patient's cells from a pre-treatment sample. The Beacon thanks a representative from Sequenta, the company that developed the deep sequencing assay that was used in the Spanish study, for reaching out to The Beacon to clarify this point.
Article printed from The Myeloma Beacon: https://myelomabeacon.org
URL to article: https://myelomabeacon.org/news/2014/04/08/minimal-residual-disease-deep-sequencing-prognosis-multiple-myeloma/
URLs in this post:
[1] minimal residual disease: https://myelomabeacon.org/tag/minimal-residual-disease/
[2] Beacon : https://myelomabeacon.org/news/2013/06/21/two-studies-investigate-minimal-residual-disease-multiple-myeloma/
[3] Image: https://myelomabeacon.org/wp-content/uploads/2014/04/MRDSurvival.png
[4] abstract: http://bloodjournal.hematologylibrary.org/content/early/2014/03/19/blood-2014-01-550020.abstract
Click here to print.