
Addition Of Zolinza Slightly Improves Velcade Treatment For Relapsed Myeloma Patients

Results of a recent international Phase 3 study demonstrate that the addition of Zolinza to Velcade increases response rates and slightly improves progression-free survival in relapsed and refractory myeloma patients compared to treatment with Velcade alone.
Specifically, 56 percent of patients responded to treatment with Zolinza (vorinostat) plus Velcade (bortezomib) compared to 41 percent of patients treated with Velcade plus placebo.
However, despite improvements in responses, the difference in progression-free survival between the two treatment groups was small. Treatment with Zolinza plus Velcade was associated with a 25-day increase in progression-free survival compared to treatment with Velcade plus placebo (from 6.8 months to 7.6 months), which according to the investigators suggests that the observed responses were not durable.
The investigators also note that although the difference in these time spans was statistically significant, it is not clear that it is clinically significant.
The share of patients who experienced severe to life-threatening side effects was similar in both treatment groups, although patients treated with Zolinza plus Velcade had more blood-related side effects. Patients in the Zolinza plus Velcade group also experienced two times as much severe diarrhea and nausea and three times as much fatigue as patients in the Velcade plus placebo group.
Nevertheless the investigators describe the side effects as manageable because patients could tolerate the combination regimen for a prolonged time with the appropriate dose modifications. They suggest that different treatment schedules for Zolinza and Velcade may decrease the side effects of the combination and, therefore, increase its efficacy.
However, Dr. Ravi Vij from Washington University School of Medicine, who was not involved in the study, doubts that an alternative schedule will be explored in clinical trials.
“At this time, I think very few physicians are prescribing Zolinza for patients with myeloma,” said Dr. Vij. “Also, Merck [the company that markets Zolinza], I believe, has decided not to file for FDA approval despite the trial being reported as positive. I think the toxicity of the combination makes it unappealing.”
According to Dr. Vij, the future of the class of drugs that Zolinza belongs to, called histone deacetylase (HDAC) inhibitors, in multiple myeloma depends to a large extent on the results of the so-called PANORAMA-1 study, a Phase 3 trial that investigates the efficacy and safety of another HDAC inhibitor, panobinostat, in combination with Velcade and dexamethasone (Decadron) in relapsed multiple myeloma patients.
Preliminary results from the current study were presented at the 2011 American Society of Hematology annual meeting (see related Beacon news).
Background
Zolinza, which is marketed by the U.S. pharmaceutical company Merck, is an oral drug already approved in the United States for a certain type of lymphoma. It also is approved for a similar use in Canada and Australia, but not in Europe.
Zolinza is a HDAC inhibitor, which works by increasing the production of proteins that slow cell division and cause cell death. Two other drugs that have been investigated as potential myeloma treatments – panobinostat and Istodax (romidepsin) – belong to the same class of drugs.
Results from previous trials suggest that the addition of HDAC inhibitors may help Velcade kill myeloma cells.
Two Phase 1 clinical studies previously demonstrated the activity of the combination of Zolinza and Velcade, with a generally well-tolerated safety profile.
These results, along with the need for additional therapies to treat patients with relapsed or refractory myeloma, motivated the investigators to conduct this trial.
Study Design
The Phase 3 study included 637 relapsed and refractory multiple myeloma patients who were treated at 174 treatment centers across 31 countries from January 2009 through September 2011.
The median patient age was 62 years.
Patients in the study had received a median of two prior therapies. The three most common prior treatments were dexamethasone (85 percent of patients in the Zolinza plus Velcade group and 83 percent of patients in the Velcade plus placebo group), melphalan (Alkeran) (63 percent and 69 percent, respectively), and thalidomide (Thalomid) (52 percent and 60 percent, respectively).
In addition, 36 percent of all patients had previously received a stem cell transplant. About one quarter (24 percent) of all patients were previously treated with Velcade, but none were resistant (refractory) to the drug.
Half of the participants in this study received 400 mg of Zolinza on days 1 to 14 and 1.3 mg/m2 of Velcade on days 1, 4, 8, and 11 of a 21-day treatment cycle. The other half received Velcade plus placebo.
The median follow-up time was 14.2 months.
Results
More patients receiving the Zolinza plus Velcade combination responded to treatment (56 percent) than patients receiving Velcade alone (41 percent).
More specifically, 8 percent of patients in the Zolinza plus Velcade group achieved a complete response and 48 percent a partial response, while 5 percent of patients in the Velcade only group achieved a complete response and 35 percent a partial response. In addition, 15 percent of the Zolinza plus Velcade group and 13 percent of the Velcade only group achieved a minimum response.
Patients treated with Zolinza and Velcade responded more quickly to treatment (36 days) than those treated with Velcade alone (43 days).
In addition, progression-free survival time was longer in patients who received Zolinza plus Velcade (7.6 months) than in patients treated with Velcade alone (6.8 months).
The study investigators note significant treatment-dependent differences in progression-free survival in favor of Zolinza plus Velcade treatment for patients without previous Velcade or Kyprolis (carfilzomib) treatment, patients with previous thalidomide or Revlimid (lenalidomide) treatment, patients with non-refractory disease, patients younger than 65 years, women, patients with less advanced myeloma, and patients with only one previous treatment regimen.
Click on image to view a larger version of it.
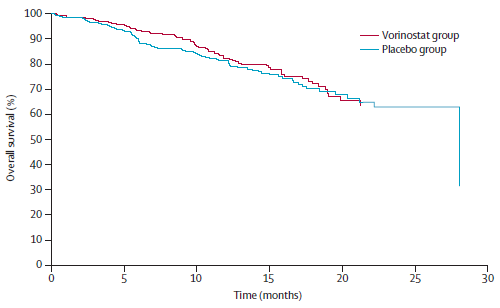
Overall survival was similar for the two groups, with a median overall survival time of 28 months for patients in the Velcade only group and the median overall survival not yet being reached for the Zolinza plus Velcade treatment group.
(Click here or on the image to the right to see a larger graph of the overall survival results.)
The share of patients who experienced severe to live-threatening side effects was similar for both treatment groups (41 percent of patients in the Zolinza plus Velcade group and 43 percent in the Velcade only group).
However, more patients in the Zolinza plus Velcade group than in the Velcade group experienced blood-related side effects. The most common of these were low platelet counts (45 percent versus 24 percent), low white blood cell counts (29 percent versus 25 percent), and anemia (17 percent versus 13 percent).
The investigators also note increases in severe fatigue (17 percent versus 5 percent), diarrhea (16 percent versus 8 percent), nausea (8 percent versus 4 percent), and vomiting (7 percent versus. 4 percent) among patients in the Zolinza plus Velcade group.
Half (50 percent) of the patients in the Zolinza plus Velcade group required at least one dose reduction, compared with 25 percent of patients in the Velcade group. Overall, more patients needed Velcade dose reductions than Zolinza or placebo reductions. More patients (63 percent) in the Zolinza plus Velcade group needed at least one Velcade dose reduction than did patients in the Velcade only group (49 percent).
The share of patients who discontinued treatment due to side effects was almost the same in both treatment groups (21 percent of the Zolinza plus Velcade group and 22 percent of the Velcade only group). Also similar was the proportion of patients who died due to complications of side effects (3 percent of the Zolinza plus Velcade group and 5 percent of the Velcade group).
When the data was collected in September 2011 for the analysis, 7 percent of patients remained on treatment and 93 percent had discontinued treatment.
For more information, please refer to the study in The Lancet Oncology (abstract).
Related Articles:
- None Found
The graph indicates to me that I, as a myeloma patient, would not choose the Zolinza addition to the Velcade therapy. Also the list of extra side effects, and the large number of patients who had to have dose adjustments to minimize those effects pretty much says no to Zolinza.
Thanks for the information on this trial. It's too bad there is not another weapon for the MM arsenal.
'According to Dr. Vij, the future of the class of drugs that Zolinza belongs to, called histone deacetylase (HDAC) inhibitors, in multiple myeloma depends to a large extent on the results of the so-called PANORAMA-1 study, a Phase 3 trial that investigates the efficacy and safety of another HDAC inhibitor, panobinostat, in combination with Velcade and dexamethasone (Decadron) in relapsed multiple myeloma patients.'
Whereas the study with Zolinza was with 58 patients, the study with Panobinostat (Panorama 1), which is a five year study ending in March 2014, was a really large study! It has been held in 212 locations, in about 35 countries. It is no longer enrolling patients...the countries for the studies were the UK, the US, Turkey , tHAiland, Taiwan, Sweden, Spain, SA, Singapore, Russia, Poland Norway, Netherlands, Mexico, Lebanon, Korea, Japan, Italy, Israel, Hong Kong, Greece, Germany, France , Finland, Egypt, Denmark, Czech Rep., China, Can., Brazil, Belgium, Austria, AU, Argentina. Wow...hope the results are good, and that HDAC Inhibitors can be included into the types of drugs effective against MM.
Thanks for your comments, Eric and Nancy.
Please note that the Zolinza trial discussed in the article above was actually quite large by the standards of what is common for multiple myeloma. As was mentioned in the article, "The Phase 3 study included 637 relapsed and refractory multiple myeloma patients who were treated at 174 treatment centers across 31 countries from January 2009 through September 2011."
The fact that it was such a large multicenter trial, with a placebo-controlled arm (with double-blinding), means that the results of the trial carry quite a bit of weight.
Sorry, I missed reading the key sentence about the 637 patients in 31 countries for the zolinza trial. There must be a lot of high hopes for this type of drug if two really large studies have been conducted, though.
Two things about the survival graph accompanying this article are bothersome. First, survival in the placebo group apparently declines about 30% in month 28. This is not a trivial number. There would have been 318 patients in that arm so 30% of that number would be 90 - 100 patients dying in that month. Am I reading this correctly? Second, results from the Zolinza group appear to lag behind results from the placebo group by about 7 months. Is this an artifact of the way that patients were recruited into the study?
Good questions, Holt. Thanks for asking them.
The sharp drop you see in survival in the placebo group around month 28 is not the result of a large number of placebo patients dying all at once.
Instead, it is the result of the way the survival curves are calculated.
As the trial progressed, fewer and fewer patients were available to calculate long-term survival because patients dropped out of the study either because of death, or because the investigators simply couldn't contact the patients any longer.
So movements in the placebo survival curve for the period after 25 months are being determined by what happens with a very few number of patients.
In fact, the authors note that, at 25 months, only 12 patients were still being tracked (or still alive) in the Zolinza group, and only 16 in the placebo group. By 30 months, those same numbers were just 1 and 0 (zero), respectively.
Most likely, the steep drop around 28 months is due to the death of a single final placebo patient who was still being tracked.
As for the lag in the survival curve for the Zolinza group up until about month 17 or 18, this is not an artifact of enrollment times. Survival in the trial was calculated for all patients as the time from when they were randomly selected to receive either Zolinza plus Velcade or placebo plus Velcade.
The lag means that, for the first 17-18 months, the combination of Zolinza and Velcade appears to offer better overall survival than Velcade alone.
The authors do not report, however, whether the difference in the two curves is statistically significant.
Thanks for the responses. It's disconcerting to learn how few patients were still being tracked in the later stages of the trial and surprising that results from so few patients are even worth reporting.