
Multiple Myeloma Survival Increased Significantly The Past 15 Years, But Unevenly Across Ethnic And Age Groups

Researchers recently reported updated survival rates for multiple myeloma patients in the United States. The results show that survival has improved steadily – and markedly – from 1998 to 2009.
The average newly diagnosed myeloma patient 15 years ago, for example, was about one-third as likely as someone without myeloma to live another five years.
By the end of the 2000s, in contrast, that same myeloma patient would be 45 percent as likely as someone without myeloma to live another five years.
Ten-year myeloma survival rates also increased markedly. However, the average newly diagnosed myeloma patient in the late 2000s was still only 25 percent as likely to live an additional ten years as a member of the general population.
Although the new study traces overall trends in survival, its focus is on trends in survival by ethnicity and age.
|
Newly diagnosed? Click here to receive an emailed copy of each new article at The Myeloma Beacon within hours of when it is published. |
The study authors report that Non-Hispanic whites experienced the greatest improvements in survival in the period covered by their study, followed by African-Americans and Hispanics. The survival of Asian and Pacific Islanders also improved, but not as much as in the other ethnic groups.
The findings indicate that myeloma patients belonging to ethnic minorities have not benefited as much from new myeloma treatments as non-Hispanic whites. The researchers argue that unequal access to new treatment options, due to lower socioeconomic status and poor or no health insurance, may explain the disparity in survival improvements.
The researchers also document in their study how myeloma survival has increased across all age groups during the past 15 years. This improvement, however, was substantially greater for patients diagnosed before the age of 70, compared to those diagnosed at older ages.
|
MORE INFORMATION News articles about: Forum discussions about: Also, see the Beacon's September 2013 update on multiple myeloma risk categories. |
Indeed, although the investigators do not emphasize the point, their findings drive home the fact that new myeloma treatments introduced during the past 15 years have primarily benefited younger myeloma patients. Improvements in the survival of older myeloma patients have been much more limited, and the survival of older myeloma patients remains significantly lower than that of younger patients.
The researchers recognize that their analysis did not account for several important factors, such as chromosomal abnormalities, stage of myeloma, prior lines of chemotherapy, and insurance coverage.
Further research is therefore needed, they write, to fully assess the impact of ethnicity and age on myeloma survival.
Background
While multiple myeloma remains a largely incurable disease, studies have shown that survival for myeloma patients has improved substantially over the last few decades. Improvements in survival occurred in the 1990s due to the wider use of stem cell transplantation, and continued in the 2000s with the introduction of novel anti-myeloma agents such as thalidomide (Thalomid), Velcade (bortezomib), Revlimid (lenalidomide).
However, according to the authors of the current study, it is not clear whether survival has increased equally across all ethnic and age groups.
Results from a previous study showed little difference in myeloma survival rates between Asians, African-Americans, and non-Hispanic whites. However, the study was based on data from patients diagnosed prior to 2003, meaning it could not address potential differences in the impact of novel agents on survival across ethnic groups.
The researchers therefore sought to assess changes in the survival of multiple myeloma patients – overall, and by ethnicity and age – in the first decade of the 21st century.
Study Design
An international group of researchers analyzed the records of 26,391 U.S. multiple myeloma patients using the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, which was started in 1973 and is now a key source of U.S. cancer statistics.
The SEER database houses information about a large sample of U.S. cancer patients, including data about each patient's type of cancer, general demographic characteristics (age, gender, and race), type of initial treatment, and survival.
The investigators included in their analysis patients with symptomatic (active) myeloma who were at least 15 years of age and who were diagnosed between 1993 and 2009. The median age of the patients included in the analysis was 67 years.
The study authors separated the patients into four groups based on their ethnicity: Asian and Pacific Islander, African-American, Hispanic, and non-Hispanic white.
In addition, the patients were separated into three age groups: 15 to 49 years old, 50 to 69 years old, and over 70 years old.
The investigators calculated myeloma survival rates for the following three time periods: 1998 to 2001, 2002 to 2005, and 2006 to 2009.
To calculate survival rates for some of the later periods, for which complete data are not yet available, the researchers made use of a modeling technique which, they say, "has been shown by extensive empirical evaluation [to provide] accurate predictions."
The survival rates calculated by the authors are what are known as relative survival rates. These are different than the survival rates typically seen in myeloma research articles, which are technically absolute survival rates.
It is common in myeloma research studies to find statements such as "The five-year survival rate was 60 percent." This (absolute) survival rate means that, five years after their myeloma diagnosis, 60 percent of the patients in the study were still alive.
The 60 percent absolute survival rate, however, does not put the survival experienced by the myeloma patients into perspective. More specifically, it does not say how many more myeloma patients died over the course of the five years compared to how many people in the general population – of the same age, gender, and ethnicity – would have died during the same period.
Relative survival rates, on the other hand, provide such perspective. They take into account that people without myeloma also die.
In particular, the relative survival rate is calculated by dividing the absolute survival rate for a group of cancer patients by the absolute survival rate for a similar group of people from the general population.
As an example, take the (fictitious) study mentioned above with the 60 percent absolute five-year survival rate. Assume that a large group of people similar in age, gender, and race to those in the study – but from the general population – would have experienced an 80 percent absolute survival rate over the same five-year period.
In that case, the relative survival rate of the myeloma patients in the study would be 75 percent (60/80=0.75, or 75 percent).
Absolute and relative survival rates will be very similar for younger myeloma patients, because younger people from the general population do not die that often. Relative survival rates for older myeloma patients, on the other hand, will be higher than their corresponding absolute survival rates.
Results

The researchers found that the five-year relative survival rate for all myeloma patients increased from 35 percent during the 1998-2001 time period, to 40 percent during 2002-2005, and to 45 percent during 2006-2009 (see graph on the right).
The investigators observed a similar trend for the ten-year relative survival rate. It increased from 16 percent during the 1998-2001 time period, to 20 percent during 2002-2005, and to 25 percent during 2006-2009.
However, the investigators noted differences in the survival rate changes experienced over time by different ethnic groups.
Non-Hispanic white myeloma patients had the highest change in five-year survival rate from 1998 to 2009 (9 percent), followed by African-American patients (8 percent), Hispanic patients (7 percent), and Asian and Pacific Islander patients (6 percent).
In the latest time period, and after adjustment for age distribution differences across ethnic groups, the five-year relative survival rates were 45 percent for non-Hispanic whites, 42 percent for African-Americans, 40 percent for Hispanics, and 43 percent for Asian and Pacific Islanders.
The most recent ten-year relative survival rates were 25 percent for non-Hispanic whites, 22 percent for African-Americans, 22 percent for Hispanics, and 28 percent for Asian and Pacific Islanders.
According to the researchers, there is currently no evidence that novel agents are less effective in minority patients. They therefore speculate that lack of access to these treatments – and, more broadly, to state-of-the-art medical care – may have contributed to the lower increases in survival among minority myeloma patients.
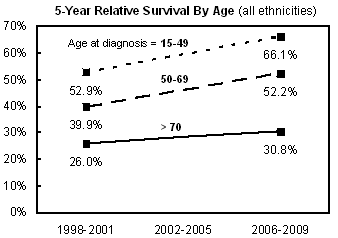
The investigators also found that younger patients had higher survival rates and greater improvements in survival rates over the past 15 years, compared to older patients (see graph to the right).
Specifically, patients who were diagnosed between 15 years and 49 years of age had the highest five-year relative survival rate in the most recent time period (66 percent), followed by those who were diagnosed between 50 years and 69 years of age (52 percent), and those who were diagnosed when they were at least 70 years of age (31 percent).
The increases over time in the five-year relative survival rates were similar among patients younger than 50 years of age and patients between 50 years and 69 years of age (13 percent for both). However, the increase was much smaller for patients 70 years of age and older (5 percent).
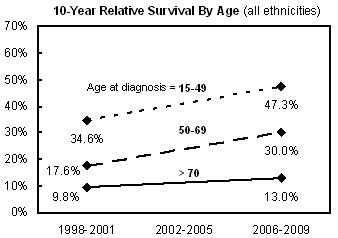
The ten-year relative survival rates in the most recent period were 47 percent for the youngest age group, 30 percent for the middle age group, and 13 percent for the oldest age group (see graph to the right).
The researchers once again observed improvements over time when looking at trends in the ten-year survival rates, although improvements were heavily concentrated among younger myeloma patients. The ten-year survival rate increased 13 percent for patients younger than 50 years of age, 12 percent for patients between 50 years and 69 years, and just 3 percent for patients 70 years and older.
For more information, please see the study in the journal Leukemia and Lymphoma (abstract).
Related Articles:
- None Found
Thanks for this interesting article. Although the study limits itself to the US, probably due to the availability of data from SEER, it would be applicable to any zone where there was uneven distribution of medical resources. The survival rates must be improving due to the better treatments available. When I was diagnosed four years ago, some people told me of their loved ones had had myeloma and really hadn't done very well at all. The whole scenario seemed depressing, and yet people I have met with myeloma are surviving longer than before. In our support group we lose people to myeloma, and yet some are still doing OK after the four years I have know them.
The study didn't differentiate on a number of factors, including gender! I wonder if there is a difference in survival there. Although the rates are not stellar of survival, still the graphs are trending upwards.
Thanks for your comments, Nancy.
The trends seen in this study for the U.S. are probably similar to those you would see in similar data for other countries. The level of the U.S. relative survival rates, compared to those elsewhere, will probably differ, for at least two reasons.
First, the introduction and uptake of the newer myeloma agents has been different in the U.S. versus other countries.
Second, because these are relative survival rates, the health of the general population plays a part in the calculation, and that differs between the U.S. and other countries as well.
Interesting that you should raise the question of gender and its impact on survival. The study reviewed in this article does not pursue that point, but we've looked at it a bit ourselves. Here is a graph of U.S. five-year relative myeloma survival rates, by gender, from 1975 to 2005 (where the year is the year of diagnosis).

As you'll see, relative survival for U.S. male myeloma patients has been consistently higher than for their female counterparts since the mid 1990s, although the gap has narrowed in recent years.
Yes, that is interesting about the gender 'gap'. It's a bit difficult to express this, but I wonder if some of the treatment regimens are more difficult for a female to withstand! There must be calculations based on body weight as to how much dosage to give a person for chemo, etc. When I compared myself to male friends undergoing the same chemo as me (I know you shouldn't make direct comparisons, but it's human nature to do so I guess), my system could not withstand as strong dose of revlimid without getting quite neutropenic. I never took more than 10 mg, and yet that was sometimes too strong!! So based on that experience, I seriously doubted whether I could have withstood a double transplant, for example. So I guess my experience told me that I wasn't as robust in some ways as some of my male friends! This is not scientific on my part, just sort of intuitive, and I am sure that many female patients are on full doses of various chemo regimes! Hopefully the gap is closing between survival rates for all of us, and the survival rates are improving too, for those of us fortunate enough to have had access to the best treatments.
Hi Navneet,
Why do you say that the Asian American survival rates are lower than the other groups? When I was reading your summary, that confounded me, and even more so when I looked at the data.
Isn't the adjusted rates looking at 5-year relative survival showing 43% for Asians, compared to 45% for non-Hispanic whites, 42% for African-Americans, and 40% for Hispanics? Likewise, the most recent 10 year survival data is 28% for Asian Americans, 25% for non-Hispanic whites, and 22% for African-Americans and Hispanics.
It is true that changes in the survival rates in Asian-Americans have improved the least over this period of time, but the likely explanation for that is that their survival rates were already a little bit better, even as far back as 1998, hence resulting is a smaller improvement score.
At least, that's how I read the data.
Alex, I don't see anywhere in the article where it says that Asian American survival rates "are lower than the other groups" (which what you say the article says). In the introduction, they write that "The survival of Asian and Pacific Islanders also improved, but not as much as in the other ethnic groups." That's a statement about changes in survival rates over time, not a comparison of survival rates at any specific point in time.
Maybe I'm missing a separate statement on the issue, somewhere else in the article. But right now I'm not seeing anything that matches up with your statement.
Hi Cyril,
My apologies. I actually wrote the comment while I a hurry, and did not state it correctly. Let me say it again, more succinctly and correctly this time.
One of the conclusions above was that the survival rate improvements in Asian Americans are lower than the other groups, and the authors surmised that the lower improvements in the minority groups might be due to unequal access to cutting edge treatments. I'm not sure that I am in complete agreement with this conclusion, and my point was that Asian Americans have the highest 10 year survival rates of all the groups. So, while their improvements over the years might have been the least, I find it difficult to attribute this to disparate access to healthcare, since they now have the highest 10-year survival. I am just trying to understand the data. That's all.
Thank you for giving me the opportunity to explain myself better!
Alex
It would stand to reason that since the other ethnic groups lagged behind Asian Americans, that as they closed the gap they would show higher improvement rates. That is simply because they had further to go especially the Hispanic and Black patients. Thus a reverse implication. Asian Americans may have had better access than other groups as a whole in prior years and now that gap is closing.
Ron
Ron,
I agree, but from at least the summary as presented here, the implications are that:
1. Asians have the least improvement rates
2. Low improvements are due to unequal access to cutting edge meds and care.
That doesn't seem to be the case at all when you look at the actual numbers. Asian-Americans already seem to have one of the best survival rates to begin with, and while this number has improved with the advent of better meds, it's lower compared to the others because of the already higher starting point of comparison.
It would be interesting to see if it's better access in the prior years, or genetics.
Thanks for this article and for the additional data on male/female differences in survival.
About the male/female data, here are some thoughts from my side.
Prior to the mid-1980s, it looks like men has typically worse relative survival than women. Then, from about the mid-1980s to the mid-1990s, men had a slightly better survival, after which the gap really expanded, until it started to shrink after 2000 or 2001.
What's interesting is that I believe these periods correspond almost exactly to changes in the treatment of multiple myeloma, and they suggest that men may respond better to treatment with melphalan than women.
If I'm not mistaken, melphalan began to be used to treat myeloma in the early 1980s. Initially, it was used as it is still used in Europe in older patients -- as part of initial therapy, not in high doses.
Then, in the early to mid 1990s, there was an expansion of transplantation for myeloma, which depends on high-dose melphalan.
Finally, after about 2000 or 2001, you saw the introduction of the first novel myeloma agents, first thalidomide, then Velcade and Revlimid, and eventually a reduced focus on transplantation as part of initial therapy.
So melphalan, for whatever reason, seems to be an agent that men respond better to than women, while novel agents tend to equalize survival rates.
Alex,
I read it the same as you.
It seemed author had a point he wanted to make but data didn't support his conclusion completely. But he made his point regardless of the results.
If he left out Asian data, the results would have supported his conclusion.
Bias creeps into these studies in many ways!
(I'd also add that I spent many a week in transplant floors with uninsured patients who appeared to have very good "access" to the newest treatments).
Nancy- my experience has been the same as what you have observed. Men I've known with mm seem to tolerate these drugs better than the women. (Sample size of 6).
If you took your average 150 pound 50 year old man and 150 pound 50 year old women and had them both drink a 12 pack of beer, I'd think the man would recover faster. Probably a stretch to equate to chemo-but not that big of a stretch.
Another reason for differences between genders and different ethnic groups that occurred to me is that sometimes people basically refuse treatment because they are so scared of the chemo and its side effects. If they have had relatives or friends suffer from cancer, take a lot of chemo, and still not do well, they just reject the whole idea of treatment. I am glad I did accept the treatments I did , since I actually have done well to date on them, even though it all wasn't very easy at times! And of course I may need more treatments in the future..that's the nature of MM.
Whether or not this could be tied into a study on different groups, I don't know. It would be more of a questionnaire type study I guess, asking people about their attitudes towards the medical professions. Also if people are not in the habit of going to a doctor for problems, or if their myeloma is not diagnosed, or misdiagnosed for some time, then they may have worse problems with their disease.
I suppose that this doesn't necessarily take away from the implied premise that some groups of people are not getting as good care as others. I think that this would have to be investigated on a wider scale, i.e. are some groups getting better medical care consistently than others vs. is this an actual problem of our biology, as I wonder about in the studies on women patients. A study like this could take in other countries where there is universal health care, to see if the same stats were found.
Nancy--that's a good point. Lack of education which is more prevalent in some ethnic groups, makes those people more distrustful of the system and/or the idea of chemo. But the care is more or less there, isn't it? Yes, you can lose your house and all, but I think the care is available. (based on observation, nothing else)
I work with a lot of mexican immigrants who have quite a lot of superstitious beliefs. (I assume it stems from the Mayan culture?). My foreman was sending $400/month to a healer in mexico who was "removing the bad spirit that dwelled inside his wife, causing her stomach problems". After 4 months he was broke but his wife's stomach was better.
In some cases, I think it's the old "leading a horse to water but can't make them drink" for lack of care.
And also, if you are looking at a donor allotransplant, unless you are caucasion, the chances of finding a matching donor are very, very slim.
Hi Stann, I didn't mean to imply anything about any particular group of people. I think it's sad when people trust faith healers more than medical professionals, but that is my bias only.
HI Nancy,
I wasn't trying to drag you into a race thing.
But it is a fact that if you want a non related donor transplant, the odds of finding a matching donor if you are african american or hispanic are very small. I learned that while my hispanic roommate at UCSF, who needed a donor cell transplant was being told that by the doctor. It was very sad to be there.
I assume it's because Caucasians sign up in greater numbers to donate than some minority groups.
Hi Stann, I don't know enough about the 'Be the Match' program to comment on that. My family, except for me since having been a cancer patient, are eligible and I think they are in it. We are a 'mixed race' family! If you look around you in Calgary, we are very multicultural, and I am sure that lots of people sign up for these programs since they are promoted by Cdn. Blood Services. So that would be a positive for matches for allogenic transplants. I think that the patients who are just desperate for the stem cells are the leukemia patients, since they cannot do an autogenic transplant at all. But of course myeloma patients are quite interested in allo transplants too, for reasons that have been really thoroughly explained in the Beacon.
But isn't it odd that the gender type doesn't seem to matter for allo transplants. I have read accounts of male alllogenic patients getting a match from a female patient, and probably the opposite is true too.
I think that misunderstandings can arise in ''social media' and I also strive not to be misunderstood (don't always succeed in that probably.)
Stann is right about the point of minorities having a difficult time finding a match for an allogeneic transplant.
"The chances of finding a matched unrelated donor improve each year, as more volunteers sign up. Today, about half of white people who need a stem cell transplant may find a perfect match among unrelated donors. This drops to about 1 out of 10 people in other ethnic groups, mostly because their HLA types are more diverse and they are less likely to take part in donor registries."
http://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/bonemarrowandperipheralbloodstemcelltransplant/stem-cell-transplant-allogeneic-transplant
It was a great thing that Robin Roberts brought attention to this issue after she was diagnosed with MDS. There were reports that more minorities went on the Be The Match Registry after hearing about it. My Doctor says there is nothing more frustrating as a physician than having a patient that wants to try and be cured of their blood cancer and not being able to come up with a suitable donor. Fortunately haplo identical and cord blood transplants are progressing as options so more patients have the opportunity to pursue curative therapy.
Mark
Yes, good you weighed in on this topic, Mark! I see that on 'One Match' (Cdn. Blood Services version of your 'Be the Match'), they are especially looking for 'ethnic males aged 17 to 35'. So if anyone reading who is an eligible potential donor to literally save someone's life by donating stem cells can register in their home country, that's great!
Hi Nancy,
As you know I used a matched unrelated donor for my allo. My donor has given me great hope for the future and a great quality of life. Stem cell donors are true heroes IMO.
I would also like to point out the value of donating blood as well. I am surprised at how many patients I meet that need transfusions and have younger family members that do not donate blood. I will never forget what I saw one day while harvesting for my auto. A young lady walked in and said she was there to donate blood for her mother. She was told that there was no guarantee that the cells would go to her Mother. She replied she would rather not bother since that was the case. Her mother is lucky everyone is not as selfish as her daughter is.
Mark
Hi Mark, I think that the patient's daughter may have been confused about donating blood for a family member. Sometimes patients bank blood for themselves before an operation. Of course, we blood cancer patients couldn't do that!
When I used to donate blood I often went with a friend. We felt it was something tangible that we could do for our health care system, and at no financial cost to ourselves either. I also used to see friends there who worked for CBS...so it was a sociable event. We were always given refreshments after donating. i quit donating a couple of years before my dx, fortunately in retrospect. iT's funny, but when the 'tea ladies' come by when I am waiting for an app't at the cancer ctr., it is reminiscent of the times I gave blood...they serve tea, coffee, juice and packaged cookies!
Many corporations run blood donor clinics, communities have them, and the blood donation clinics cast a wide net to get donors. It is a valuable system in our world of modern medicine, don't you think?
Interesting information, however it is a little confusing because to have a 10 year survival for years 2006 through 2009 you would have to have data through the end of 2016 through 2019. In addition, the last published data from SEER show only the 2005 5 year survival rate so how can anyone have data for 5 or 10 years after 2005. They are usually 2 to 3 years behind. They must have done a lot of estimating! I can believe the first two points of the 5 year graph and the first data point on the 10 year graph. Directionally is is probably accurate. Gary
Thanks for your comments, Gary.
Your feedback reminded us that we meant to go back and mention in the article that estimates for the later periods that extend out beyond the period covered by the SEER dataset are based on a widely-employed modeling methodology which, the authors note, "has been shown by extensive empirical evaluation [to provide] accurate predictions."
We've updated the article to include this clarification.
Also, although SEER currently publishes results only through 2005, academic researchers have access to (anonymized) individual patient-level data up to 2010. This makes it possible for researchers to develop estimates, and use modeling methods, that are not feasible using just the standard high-level results published by SEER.
A similar study that used the CIBMTR(Center for International Blood and Marrow Transplant Research) US and Canada Data Base and titled
"Trends in Utilization and Outcomes of Autologous Transplantation as Early Therapy for Multiple Myeloma" and can be found at the link: http://www.bbmt.org/article/S1083-8791(13)00351-0/abstract
This study would suggest that the Relative Survival for transplant patients is 60.6% or 45% greater than that represented in the above study. However, one caveat is the average age in this study was 57 vs 67 for the above study. This would account for 15% of the difference which would leave the transplant only study 30% better than the SEER data study.
Thanks for the additional comment, Gary.
The survival results in the SEER study described in the article above, and those in the CIBMTR study you mention, actually agree quite well. You just have to be careful that you get as close to an apples-to-apples comparison as possible.
This is going to get a bit detailed, so bear with us.
In the SEER study, the 5-year relative survival of all myeloma patients diagnosed from 2006 to 2009, and age 50-69 at diagnosis, was 52.2 percent (this is in the second graph above). "All" myeloma patients means all the myeloma patients in the database, regardless of disease severity, transplant eligibility, and race.
The CIBMTR study looks at survival results for patients who had a transplant within one year of diagnosis. It measures absolute, not relative, 5-year survival from time of transplant. And it includes results for patients who had their first myeloma therapy from 2005 to 2010. Those patients had a median age of 58.
On that basis, the CIBMTR study finds a 5-year survival rate of 57 percent (compared to 52.2 percent for the closest comparable number from the SEER study).
Now, given that the SEER study above looks at all myeloma patients, not just transplant-eligible patients, and given slight differences in time periods covered, survival measures used, and ages of the different groups, we'd say the results of the two studies are actually rather comparable.
Bear in mind, as well, that the SEER study uses much more comprehensive data than the CIBMTR study.
The SEER looks at survival outcomes for a total of 26,391 patients diagnosed between 1998 and 2009. The survival results in the CIBMTR study, in contrast, are based on just 4,373 patients diagnosed over a longer period (1995 and 2010).
The Beacon covered the CIBMTR study in detail when its results were presented at the last ASH meeting. Here's a link to that article about it:
http://www.myelomabeacon.com/news/2013/01/22/stem-cell-transplantation-trends-for-multiple-myeloma-ash-2012/
The article also includes a link to a PDF file with the Powerpoint slides from the presentation. The slides were provided as a courtesy to the Beacon's readers by Dr. Luciano Costa, the lead author of the CIBMTR study. Here's that link:
http://static9.light-kr.com/documents/Costa%20-%20ASH%202012%20-%20ASCT%20Trends.pdf
I overlooked your second graph and it would be more comparable, however the CIBMTR data would have to be adjusted to account for the difference from there use of Overall survival versus that represented by the SEER data base which is Relative survival, which excludes non myeloma deaths. My estimated adjustment would be to increase the CIBMTR number by 3.6% to 60.6%. So the numbers now are much closer but would still reflect that a CIBMTR SCT would be 17 percent better than survival at the average SEER facility which includes both transplant and non transplant.
Finally, you mentioned that the CIBMTR was based on 4373 patients, however the article lists 20278.
What both groups of data continue to highlight is the vast difference in survival rates between the best multiple myeloma specialist(10+years), and the average SEER facility which is less than 5 years.
Thanks for the additional thoughts, Gary.
We agree that the CIBMTR numbers would need to be adjusted upwards, along the lines you suggested, to make the comparison more "apples to apples". However, we think there also would need to be a noticeably upward adjustment to the SEER number given that it includes patients who were not transplant eligible (and therefore likely to be less healthy), and it also probably includes an older set of patients.
The CIBMTR survival data is, in fact, based on the 4373 patients that we mentioned. Some of the statistics in the CIBMTR study are based on the larger sample of patients that you mentioned. However, the survival estimates in the study are based on the so-called "Case Report Form" (CRF) database, which covers 4373 patients from 1995 to 2010.
See slide 11 of the deck we provided a link to above for a description of the two databases used in the study, and slide 16 for the explanation that the smaller CRF database was used for the survival estimates.
We couldn't agree more that myeloma patients who get care directed by a myeloma specialist are, in most cases, likely to get better care -- and longer survival -- than if they were to stick with just their local oncologist.
Just a few more thoughts, the CIBMTR study was based on two data bases, the 4373 patients of the CRF database and the 20278 patients in the TED database. You mentioned the graph 16 and this is for the CRF database, however graph 17 shows the TED data and mirrors that of the CRF results, or the two graphs from two different data bases confirm their assertion that there has been an improvement over time and the 5 year survival is about 57%.
In addition, in the Beacon article you mentioned, it states,"Therefore, he and his colleagues analyzed data from the Center for International Blood and Marrow Transplant Research (CIBMTR) for 20,278 U.S. and Canadian myeloma patients who underwent autologous stem cell transplantation within 12 months of their diagnosis between 1995 and 2010. and Patients in Dr. Costa’s study were divided into three groups based on the time when they received their transplant: 1995 to 1999 (2,226 patients), 2000 to 2004 (6,408 patients), and 2005 to 2010 (11,644 patients)."
However, I think this is moot in that with a sample size of 4000 or 25000, both are of a sufficient size to provide an adequate representation of mean.
Just like to make hope i have been diagnosed with mm 1997 and received two stamcell transplantations. Now march 2014 i am still blessed and completly clean. Believe, prayers and an excellent oncologist Dr. Ruckser in Vienna, Austria have bring the success to me! God bless yoou all..
Get new Myeloma Beacon articles by email.